How much weight will I lose? How much weight should I lose? I was told I should lose 40 pounds. I want to fit into my clothes! I know when I was x-number-of-pounds I felt great.
What are your thoughts about your weight loss expectations? Many people beginning a weight management effort will have thoughts about a target or goal weight, and thoughts about what would be their ideal weight.
Would you be surprised to know that your weight is considered something that you do not have control over? Put simply, weight is not a behaviour. It’s not something you do. Consider for a moment the key things that affect your weight that you DO have control and influence over. When you are eating as healthily and moderately as you can while still enjoying your life in a sustainable way, and when you are as active as you can be in a sustainable way, exactly where you land with your weight is determined by an appetite system that is hundreds of thousands of years old.
Another name for your appetite system is your weight regulation system. It comprises three levels of your brain. This is where your weight is regulated; as you lose weight, the fat loss is expertly recognized by the GateKeeper in your hypothalamus, or homeostatic system. In response to weight loss, the GateKeeper will initiate changes that favour weight gain as weight loss is defended against. Specifically, your metabolic rate will decrease and WANTING via the GoGetter will increase as your motivation system becomes strengthened. These changes are the reasons for the characteristic “shape” of all successful weight loss efforts as seen below. This shape is so characteristic of almost all weight loss patterns you could think of this graph as “the shape of human weight loss.”

In a landmark review paper, Kevin Hall and Scott Kahan describe this process. Consider the shape of the above graph as a representation of the steady behavioural battle against a biological response that progressively opposes weight loss. You should know that all of this data is the product of validated mathematical models of energy expenditure applied to real weight loss seen in real humans, all with accurate gold standard metabolic rate measurement. While weight and metabolic rate are measured directly, energy intake, appetite and effort are estimated.
To explain why the shape of weight loss looks like this, the researchers used the example of a hypothetical 90-kg woman who loses weight and keeps it off. The weight loss she experiences is represented by the graph below. Note that her weight loss plateaus at approximately six to nine months.

In our example, before her weight loss effort, this hypothetical 90-kg woman was consuming an average of 2,600 calories per day and burning an average of 2,600 calories. She was consuming what she was burning and therefore her weight was stable.
The weight loss process begins with this woman dropping her calorie intake from 2,600 down to 1,800 kcal per day, thereby establishing an 800 calorie per-day deficit. This is the change that initiates her weight loss.
This next graph suggests what happens as her metabolic rate slows in response to her calorie deficit and subsequent fat loss. Look how it drops from 2,600 kcal per day to roughly 2,400 kcal per day within the first month, followed by a stabilization. This is how the GateKeeper drops the metabolic rate in defence against fat loss.

What about calories in? This is important. Increases in calories consumed is considered the most important determinant of the slowing and eventual plateauing of weight loss, along with this characteristic graph shape. Look what happens to her energy intake! She starts consuming 1,800 calories a day, but as soon as she starts losing, she is immediately consuming more! By three months she is (often unwittingly) consuming an average of 2,200 kcal per day, a full 400 calories more a day than she was consuming when she started her weight loss! By six to nine months she is consuming an average of 2,400 calories per day.

So you see why at six to nine months her weight is plateauing. At six to nine months she is consuming 2,400 kcal per day and her metabolic rate is 2,400 kcal per day. She is consuming what she is burning and her weight loss has stopped.
The next curve is very telling. This is the answer to why this woman was driven to eat more as soon as she started to lose weight. This graph shows the actual changes in her appetite. The appetite here is defined as the number of calories her brain would prefer her to be eating each day to regain the weight she lost. This graph shows that in response to weight loss, appetite and therefore intake immediately increase. Think of this as the GateKeeper recognizing fat loss and making the GoGetter (appetite) work harder.


What follows may seem a bit confusing but it is worth trying to understand because this is actually what happens. At first our hypothetical woman was eating 1,800 kcal per day and her appetite was asking for 2,600 kcal per day, so her effort was that of eating 800 kcal less each day than her brain—her appetite—would prefer. By three months in, her appetite is at 3,000 kcal per day, and you will remember at three months she was eating on average 2,200 kcal per day. This means that her effort at three months was the same as at the beginning: she was taking in 800 kcal less than her brain was asking for (but because she was eating more, her weight loss was already slowing). At six to nine months her brain is asking for 3,200 kcal per day (again the work of the GateKeeper and the GoGetter) while she is eating 2,400 kcal per day. Again her effort at six to nine months is the same: she is eating 800 kcal less than her appetite was dictating. At this point, though, because she is eating 2,400 kcal per day on average, her weight loss has plateaued.
This final graph demonstrated the point of adherence to effort. Here we see that to sustain weight loss calls for a sustained effort. In this graph the effort level is defined as taking in 800 calories less than your brain desires long into the future.

So now you see that when you are beginning a behavioural weight loss program, it is suggested that you consider establishing a level of effort that is sustainable over the long term.
As the graph shows, when you are doing the best you can, at an effort level you can maintain, exactly where your weight lands is determined by the response to weight loss within you; your appetite system, which regulates appetite and metabolic rate. This is what it means when it is implied that you do not control your weight. You control, at best, your behaviours and effort. When you are doing the best you can do… your weight lands at a BEST WEIGHT. This graph shows that someone losing weight and keeping it off is practicing the same level of effort long into the future.

You now understand that often, at around 6-9 months after beginning to lose weight, calorie intake will increase to the point where the number of calories consumed matches the number of calories burned. When this happens, weight loss stops, defining the characteristic weight loss plateau.
In this scenario you work on finding your 1) most modest, 2) yet enjoyable, and 3) sustainable lifestyle, and then you stand back and let your brain and body “tell you” where your best effort lands you.
In the above scenario there are two competing processes: 1) your brain defends your former weight while 2) you defend your BEST WEIGHT. Many people at this point will ask “does the brain ever give up trying to return you to your original higher weight—does it ever let up in its effort eventually? After all, does it not prefer you to be at a healthier weight?” Unfortunately, at this point we have no evidence of the brain letting up in either increased appetite or decreased metabolic rate.
You will read repeatedly in this material that overweight and obesity is a real medical condition that is primarily genetically conferred, progressive and centred in the brain. These concepts are very well illustrated here. Genetics determines the degree to which your brain defends against weight loss; the degree of increased appetite and the degree of decreased metabolic rate. Yes, this means that weight loss results will necessarily be unique to you. Understand that all the graphs above from the Kevin Hall review paper are taken from an average of thousands of subjects. Your results can be very different in either direction. This is why the concept of a predetermined target weight, ideal weight or goal weight makes no sense at all.
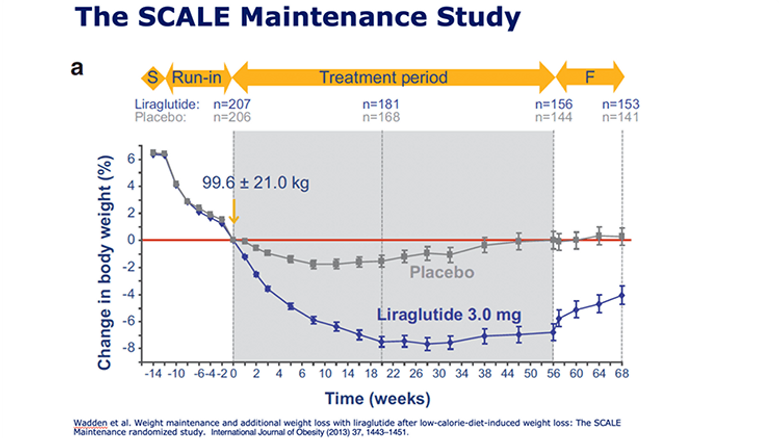
This is a really important point. If you are engaged exclusively in a comprehensive behavioural weight management program and you reach a plateau, further weight loss is possible and probable. It is extremely common and will continue to become even more common to see a behavioural program combined with a weight loss medication, also called an anti-obesity medication or AOM. AOMs can be very effective at creating a lower BEST WEIGHT. See this graph from a study called the Scale Maintenance Study. Here, after 12 weeks of losing weight with a diet, subjects were randomized to either a placebo or an AOM. What you see is that the two subsequent weight loss curves are the same shape but that the weight loss in the AOM group is deeper. You will remember that appetite and weight are regulated in parts of the brain (GateKeeper and GoGetter) that we do not have access to, but AOMs do. Here you can think of the effect of AOMs as dampening the brain’s “weight gain favoring” response to weight loss; hence, AOMs support weight loss. The GateKeeper becomes less alarmed by fat losses and the GoGetter becomes less sensitive to cues and WANTING decreases.
If further weight loss would improve health and quality of life and yet you believe that you cannot realistically eat less at a sustainable effort, the addition of an AOM can be tremendously sensible. Currently, there are AOMs that are available, safe and effective. The effectiveness of AOMs—specifically, the average percentage of body weight loss achieved—is advancing significantly. The use of AOMs will be much more common and better understood in the near future, and AOMs should be an option for anyone who qualifies and is interested.
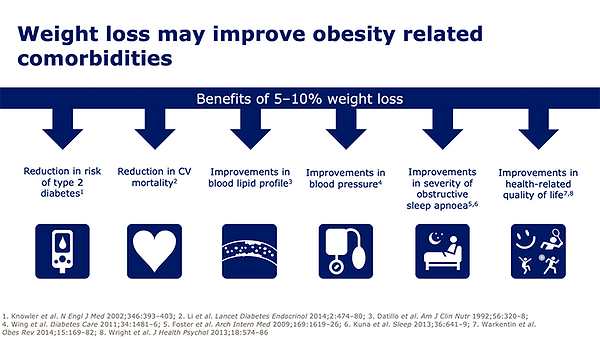
A sustained weight loss of as little as 5%–15% results in clinically significant health benefits. These benefits include substantial reductions in deaths from heart disease and stroke, reductions in heart disease risk factors (high blood pressure and high cholesterol), improvement in or remission of diabetes, improvements in conditions such as sleep apnea, fatty liver and osteoarthritis. A 5%–15% body weight loss also importantly results in significant improvements in health-related quality of life. Larger percentages of weight loss have been shown to reduce the risks of a series of 11 cancers.
A common goal of weight loss is to feel better about how one looks. A common expectation is that weight loss always results in improved body satisfaction, and the more weight that is lost the happier one will feel. Would you be surprised to know that this is regularly untrue? Simply put, how you feel about yourself can be inconsistent with how you look. Many people who are thin or of average weight dislike their appearance or are dissatisfied with certain parts of their body. Many people who are heavy feel attractive and comfortable with their appearance.
The subject of body dissatisfaction, and the work involved in addressing it, is covered in the final section of the Resilience module. Briefly, body satisfaction is more about the beliefs you hold about your body than it is about the size of your body. These beliefs are shaped primarily from external messages that you have received about body shape from sources ranging from our weight-obsessed culture to your family, coaches and friends. Body satisfaction is about being more accepting and less critical of how you look. Those who have or achieve body satisfaction will describe that some aspects of their appearance they like and some aspects of their appearance they tolerate, but most importantly they spend minimal time focused on their image and more free to focus on other things.