At its most basic level, weight gain occurs when calorie intake exceeds calories expended. Conversely, weight loss only occurs when energy intake is less than total calories burned. Weight loss occurs when calorie intake is reduced, regardless of the percentages of fat, protein or carbohydrates eaten. Calorie intake, not carbohydrate intake, is the determinant of body fat gain or loss. At this point, the calorie content of food is literally the only food property that has ever been convincingly demonstrated to impact how much fat is carried in our bodies. This was most recently validated by a meta-analysis of 20 studies suggesting that “for all practical purposes … a calorie is a calorie” as it relates to body-fat-weight.
Studies consistently show that once heavier, heavier individuals consume and expend approximately 20%–30% more calories than lighter individuals. Studies held within tightly controlled laboratories/dormitories demonstrate that reducing calorie intake by this same number invariably causes fat losses, suggesting that higher calorie intake is required to maintain higher weights.
Weight loss happens only if our calorie intake is lower than the total number of calories we burn, but the math should not be mistaken as simply “calories in–calories out.” The math changes in predictable ways when, as discussed, the brain detects fat loss (think GateKeeper), and generates increased appetite and decreased metabolic rate to favour weight regain.

What is the best diet for weight loss? What if the answer was a resounding NONE? You will be asked to consider disregarding the debate about the optimal weight loss diet. Despite years of searching, no best diet has been found. Countless studies comparing different diets (e.g., low carbohydrate, ketogenic, low fat, intermittent fasting, Mediterranean) have shown minimal and inconsistent differences in weight loss and health outcomes. In randomized, controlled trials, low-carbohydrate and low-fat diets yield similar and very modest long-term weight loss results; weight loss differences between the two diets are “minimal” after 12 months.
“I thought carbohydrates were bad for you?” There is a decades-old popular hypothesis that says that your weight is about the carbohydrates you eat and not the calories. This hypothesis says that when you eat sugar and simple carbohydrates, your insulin levels increase, resulting in the storage of fat, increased appetite and slowed metabolism rate. This hypothesis is called The Carbohydrate-Insulin Hypothesis (CIH), and it is the theoretical basis for ALL low carb dieting, ketogenic dieting and intermittent fasting. But is it true? Fortunately, hypotheses can be tested. Is insulin the determining factor in fat gain due to its direct effect on fat cells, hunger and metabolic rate? Note, a majority of evidence is contrary to the CIH and readers are reminded to reference the Internalized Weight Bias module, where the prevailing theory of fat gain is described as a product of a collision between a unique, inherited brain-centred appetite system and our modern obesogenic food environment.
In 2012, millions of dollars were raised and the Nutrition Science Initiative (NuSI) was founded to investigate the carbohydrate-insulin hypothesis. The organizers were proponents of low carb dieting and they set out to prove the hypothesis. They organized three significant clinical trials and recruited three serious researchers: Kevin Hall, Christopher Gardner and David Ludwig. Spoiler alert: of the three published studies funded by NuSI, at least two, and possibly all three, decisively refuted the carbohydrate-insulin hypothesis.

The first studywas conducted by an impressive group of obesity researchers including Kevin Hall, Rudolph Leibel, Michael Rosenbaum and Eric Ravussin. A simple and elegant design saw 17 volunteers with overweight or obesity confined to a laboratory/dormitory for 8 weeks. Every calorie they ate was measured and provided. For the first 4 weeks they were fed a high carb–high sugar diet, and for the second 4 weeks they were fed a very low carb ketogenic diet. Metabolic rates were measured using both a chamber and something called “doubly labeled water.” Body composition was measured using the gold standard DEXA, and relevant blood markers were measured, including insulin. The results were devastating to the CIH. The high-carb diet demonstrated superior fat losses. The ketogenic diet reduced insulin levels by 50% but the rate of fat loss actually slowed, which was the opposite of what the carbohydrate-insulin hypothesis predicted.
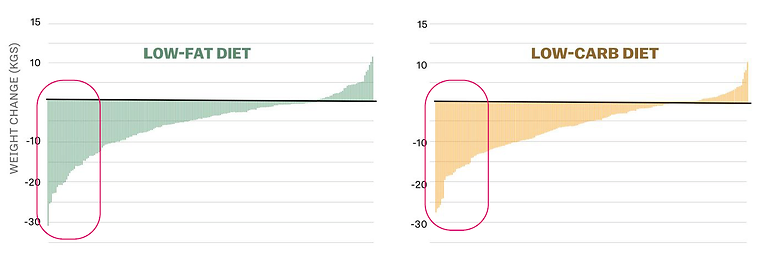
The second study was called the DIETFITS Randomized Clinical Trial. DIETFITS may be the most rigorous diet comparison study ever done. The study was conducted by the talented Stanford researcher Christopher Gardner. The study compared a whole food low-fat diet to a whole food low-carbohydrate diet in 609 subjects over a period of 12 months. Each subject attended 22 sessions with a registered dietitian; no calorie intake targets were given. The study looked to see if genotypes or insulin production predict weight loss. DEXA was used again to measure body composition, and metabolism was also measured.
What did the study find? Importantly, the study found that the two groups stuck to their assigned diets of either low carb or low fat throughout the study (this is a sign of a well-executed study). More importantly, the study showed no significant differences in weight loss between the two groups. Also, it was found that neither genetics nor insulin levels could predict weight loss.
If you look at the results in the “waterfall plot”, you can see similar results between groups and notable variances between individuals in the same group! In fact, the differences in weight loss between individuals on the same diet were much larger than the variations between diets, suggesting differences in adherence were more important than differences in diet.
The DIETFIT study served to replicate the results of numerous other randomized, controlled studies showing the proportion of fat and carbohydrates to matter very little for weight loss, again seriously challenging the carbohydrate-insulin hypothesis.
The third study compared the effects of low fat vs. low carb on metabolism through 20 weeks of weight maintenance following weight loss. Weight, insulin levels and metabolic rate were measured using the doubly labeled water technique. In support of the carbohydrate-insulin hypothesis, the authors reported that a very low-carbohydrate diet led to a higher metabolic rate than a low-fat diet. However, a reanalysis of the raw data suggests that the effect may be an artifact. As described by Kevin Hall, “analyzing the data according to the original pre-registered statistical plan resulted in no statistically significant effects of diet composition on energy expenditure.” This alternative analysis of the data is also consistent with a meta-analysis of 32 controlled studies examining the same phenomenon that found energy expenditure favoured low fat diets!
Taken together, it has been a tough few years for the science of low-carb dieting and the carbohydrate-insulin hypothesis.

Ethan Weiss, a cardiologist at UCSF, was successful losing weight using intermittent fasting but he was uncomfortable recommending it to his patients because of a lack of research with human subjects as study participants (rather than mice). Ethan decided to conduct the first-ever human randomized controlled trial comparing intermittent fasting with continuous eating. The researchers chose the 12PM–8PM window. The primary end point of the study was weight loss at 12 weeks.
The TREAT trial was published in 2020 and what did they find? According to Ethan in a popular twitter thread:
“Well, let’s start with the bottom line. This was a negative study. Intermittent fasting did not lead to a statistically significant difference in weight loss at 12 weeks.”
Again, the same type of waterfall plot shows differences between individuals but not significant differences between the continuous meal timing (CMT) and the time restricted eating (TRE).
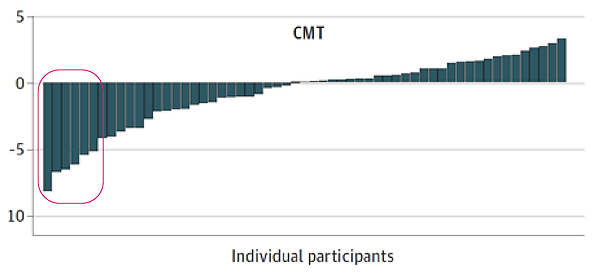
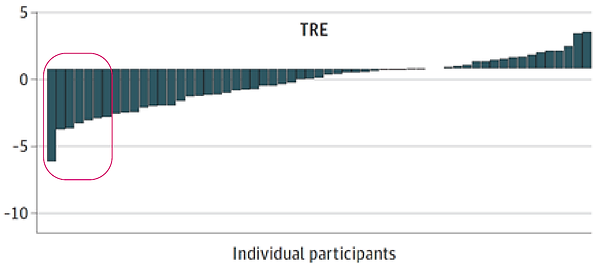
There were also no differences between groups in insulin, glucose, lipids, sleep, activity, metabolism or fat mass.
Of note, and a potential warning of harm for those considering intermittent fasting, is that the intermittent fasting group was found to lose more lean mass (muscle) than the continuous eating group.
Look at the red circles in each of the waterfall plots. Within them they contain a representation of the individuals in the trials who best maintained adherence to the behavioural changes—primarily to eating less. The only consistent finding among trials that compare diets is that adherence—the degree to which participants maintained effort and continued in the “program” was strongly associated with 1) weight loss and 2) improved health.
Can you find help with adherence? It is the fundamental role of a weight management behavioural program to support and improve adherence! Behavioural programs support adherence and therefore behavioural programs lead to greater success. This material in its entirety comprises a comprehensive behavioural program.

Eating healthily
Eating healthily promotes health of body and mind. There is minimal controversy as to what constitutes eating healthily. To eat healthily one considers a diet of minimally processed whole grains, fruits, vegetables, lean proteins, lean dairy, good fats and minimal alcohol. At the same time most of us value food +/- drinks, fun and friends, socialization, celebration and the positive and unique role food and drink play in all of these experiences. (For more information regarding healthy eating, please reference the parallel nutrition program material including “Healthy Eating: Why it Matters” and “Optimizing Nutrition: Health-Promoting Foods”.)
So, would you consider finding your own “best” diet, the healthiest eating that is realistic, enjoyable and sustainable? Importantly, the behaviours and effort level adopted to lose weight will be the same as those needed to maintain weight loss, so consider eating in a pattern and effort level that is both enjoyable and sustainable. In a parallel nutritional program, you will learn about the calorie density of foods and how to estimate portion sizes so that you can make the best assessment of your calorie intake. You will be invited to consider tracking your intake while being made aware that self-monitoring of food and drink intake is not for everyone.
Exercise
Next to quitting smoking, physical activity is the most valuable behaviour available to improve longevity, quality of life and chronic disease risk reduction. You will be encouraged in this behavioural program to be active, to identify obstacles to physical activity , and to develop skills and strategies to overcome these obstacles.
Surprisingly, studies show that exercise alone will not promote significant weight loss in most people. In an important systematic review and meta-analysis of randomized controlled trials, researchers found that moderate intensity exercise programmes of 6 to 12 months’ duration were associated with only modest improvements in weight (~4 pounds), waist circumference (~2cm) and cardiovascular risk in overweight and obese populations.
Exercise, despite its significant health and quality of life benefits, may have significant limitations in its ability to establish a calorie deficit and weight loss. In a landmark clinical trial, Herman Pontzer and colleagues show that even low levels of physical activity increase the number of calories we burn. This makes sense: the more active we are, the more calories we burn. However, the researchers found that at higher levels of activity there is no expected rise in energy expenditure and that the body adapts to maintain total energy expenditure within a narrow range. This is called the constrained model of energy expenditure. What this model suggests is that if you were to burn 400 calories today on a treadmill, in response, your body would over time burn 400 calories less than what it was going to just to make up for the extra calories that you burned! If this seems unfair, it may seem less unfair if you consider this mechanism against burning extra calories as adaptive in an environment when work was required to find food and calories could be scarce.
This information is critical to understanding the place of exercise in weight management. You will learn in the Modulators module that stress, fatigue, depressed mood and anxiety can all challenge weight loss efforts by increasing your appetite and decreasing your ability to self-regulate against WANTING. Exercise can be very beneficial because exercise clearly and positively impacts stress, fatigue and mood. In fascinating trials, exercise has been shown to potentially directly reduce WANTING signals in the brain (dampening the GoGetter).
Like best diet, you will be asked to establish your “best” activity level, the highest level of activity that is enjoyable, reasonable and sustainable. For more information on the place of exercise in weight management, please reference the exercise material “Physical Activity and Your Weight”.