We are all motivated to eat. This is a basic function of survival. Our brains are equipped with an ancient motivational system that ensures we are driven, subconsciously, to hunt and gather — to go and get — particularly calorie-dense food. This ancient system can lead to overeating and weight gain in our modern food environment.
Wanting — the motivation to GO AND GET calories
This section can be thought of as the beginning of treatment. You have already established that excessive calorie intake drives weight gain and confounds weight loss. But what drives excessive calorie intake? You might think the answer is complicated, but it isn't.
The answer lies in the middle layer of the appetite system. The appetite system has three layers, and the middle layer is best known as the motivation system. The human appetite system evolved from living in an environment where calories were often scarce and finding food involved work — hence the motivation to go and get.
The prevailing understanding1 of how and why obesity happens is that this ancient system has collided with the modern food environment: ultra-processed, sugar-fat-salt added, big-portioned, everywhere, anytime, aggressively advertised, delivered-right-to-your-front-door food. It is also important to note that even the overabundance of healthy food in our current food environment can drive the overconsumption of calories and contribute to weight gain. The assumption that weight gain, overweight, and obesity are always the result of unhealthy or highly processed junk and fast food is both flawed and highly stigmatizing.

What this collision produces
Abundant and energy-dense foods ensured survival in our former environment. When we eat abundant or tasty food, it is sensed in our mouth and digestive tract, and a signal is sent to the brain that we are eating survival-imperative foods. As the food and signals collide with our motivation system, we learn2 to associate the environmental cues around us with these foods. This is called associative learning, or Pavlovian learning. After repeated associations, the environmental cues themselves gain the power to generate WANTING, and make us go and get.
It is worth being precise about the stimulus at the centre of this, because it is specific. We can call it reward-value food: the foods the brain recognizes as important for survival — dense with calories, with sugar, with fat, with salt. Literally the makings of survival. When we eat these foods, the brain knows it. There are receptors from the mouth to the back of the throat and downward through the digestive tract, with direct lines to the brain, telling it that this is the good stuff. That signal is the engine of the learning. Enough associations between reward-value foods and the settings, cues, and circumstances that surround them — specifically the cues — and eventually the cues themselves generate the drive. What they generate is the primary symptom of obesity in the modern food environment: a motivational drive to go and get, a surge of dopamine, an activation of the mesolimbic system — incentive motivation.
Ivan Pavlov and the bell.
Ivan Pavlov was a Russian scientist in the early 1900s. You may recall his famous experiment in which dogs salivated to the sound of a bell. By repeatedly pairing the bell with the delivery of tasty sausage powder, the bell alone eventually became a powerful trigger of salivation — that is, of wanting — in the dogs. Salivation is a reflexive and automatic response to the anticipation of food, an early phase of digestion, and it was triggered by a bell. Pavlov even showed that salivation was triggered in the absence of hunger, by ringing the bell after the dogs had been fed. By mapping out your high-risk times, you are discovering your own "bell" — the settings and cues that have, in your life, been paired with tasty or abundant food repeatedly, and are now powerful triggers of wanting.
What wanting is, and where it lives
Wanting is also known as desire, urge, impulse, craving, attention bias, or incentive motivation. It is often described as a wave, because of its property of rising, cresting, and falling. Wanting resides completely in the subconscious. It happens without conscious awareness and is the driver of overeating.
For example, if abundant or tasty food is paired enough times with the setting of night-time, couch, TV, dark windows, pre-bedtime, eventually that setting itself reflexively and subconsciously generates wanting and makes you go and get. If the setting of walking through the door to your home at the end of the day — the jacket off, bag down, walk into the kitchen — is repeatedly associated with pre-dinner tasty energy-dense food or drink, eventually the simple act of walking in your door at the end of the day gains the power to generate reflexive wanting for food or drink. In these scenarios, the times of day and the environments become established as high-risk times.
Wanting is different from hunger, but both are real and powerful physiological responses. Hunger from going too long without food also triggers wanting. But wanting commonly happens without hunger — and these are the times people take in more calories than they need, because wanting drives excessive calorie intake.
Wanting is not liking
It is worth being precise about what this drive is, because it is easily confused with pleasure — and the two are not the same. Wanting and liking are dissociable: separate systems, doing separate jobs. Wanting is the drive, the motivation — the dopamine-mediated, mesolimbic surge that moves us to go and get. Liking is something else: the pleasure of the food as we actually eat it, an endocannabinoid- and opioid-based response in the brain. Liking is real, and it is necessary for the learning — the pleasure is part of how the associations get laid down in the first place. But it is not necessary for the wanting. The two come apart. Even if you took the pleasure away, the wanting would remain, because the drive is not running for the pleasure — it is running for the motivation. The symptom moves us toward food, whether or not much enjoyment is actually on offer. This is part of why wanting can arrive with no hunger, and act on us in settings that promise little real pleasure at all.
Why this drive is hard to see
This drive goes by many names — wanting, craving, desire, urge, incentive motivation, attention bias, food noise — and the sheer number of them is itself part of the difficulty. Two things, in particular, keep this principal symptom unclear to people. The first is that it lives in the subconscious: it is not a thought you can catch in the act, so it is genuinely hard to be certain you have named it correctly. The second is that there is a great deal of cultural misunderstanding around it — folk explanations, misinterpretations, the inherited mythology of willpower and emotional eating — that crowds out the simpler mechanism sitting underneath. So if the drive feels slightly out of focus even as you describe it, that is expected, and it is not a failure of understanding on your part. It is the nature of a subconscious, much-misunderstood, many-named thing. Naming it plainly, again and again, is how it comes into focus.
The diminution of wanting
When obesity medication works, what it produces is specific: a lowering of wanting. Picture a sliding scale, with high motivation — a profound interest in food — at one end, and apathy at the far extreme of the other. The medication shifts a person down that scale: reduced interest, a lowering of the drive. Usually not all the way to apathy — apathy is the far pole, not the expected destination.
Patients describe this one phenomenon in many ways: less interested. I don't want it. It's not on my mind. I'm not thinking about food as much. The food noise has quieted. I have more bandwidth, more attention. I'm good, I'm done — don't want any more. All of these refrains describe the same thing: a lower point on the scale of wanting. (It is worth noting that "food noise" is a folk term that bundles the subconscious pull together with its conscious narration — so when the noise quiets, more than one thing may be quieting.)
A second family of descriptions deserves precision: I get full sooner. I'm satisfied with less. I'm still eating the same foods, just less of them. It is natural to call this fullness — but it is not fullness. Fullness is a weak, overridable signal; we can and do eat through it. This is lowered wanting misinterpreted as satiety. The distinction matters because it keeps the mechanism in view: the change is not in the stomach's report of "enough" — it is in the drive to go and get.
The genetics of wanting
Approximately seventy percent3 of the likelihood of struggling with weight in one's lifetime is inherited. Over a thousand genes have been associated with overweight and obesity, and a majority of them are expressed in the central nervous system4 — the brain — where weight, appetite, and metabolism are regulated. The strength of the motivational drive to go and get is itself highly heritable. Stronger wanting is considered a key heritable risk5 for weight struggles.
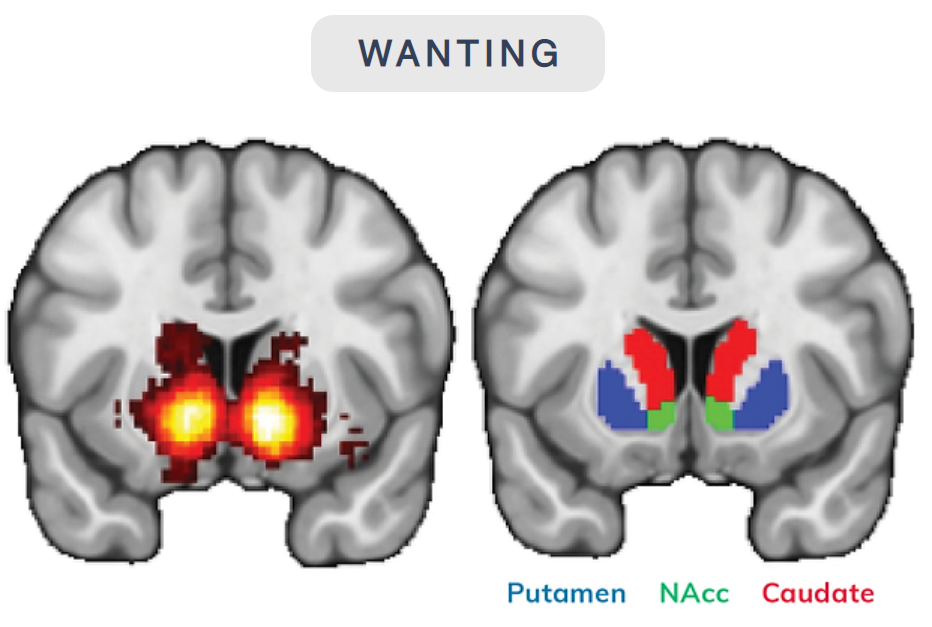
Wanting is a neurological reflexive brain event mediated by a chemical called dopamine. It can be clearly seen on functional MRI as this part of the brain lights up in response to food cues.
Mapping wanting and your high-risk times
Your wanting map contains the cues, places, times, and settings that have repeatedly been associated with abundant or tasty food or drink in the past — and where you now reflexively and subconsciously experience wanting. What are these cues?
Mapping determines your high-risk times. Consider the following exercise to help you identify yours.
Let's say this is the timeline of your day. At the beginning of the line is when you wake up; at the end is when you go to sleep. Is there anywhere along this line where you would consider yourself, with any regularity, more at risk of eating more food or drink, or less healthy food?
When it feels like "anytime" — or like stress
Some people map their high-risk times easily; others find it genuinely hard, and land on the same place: it's not really a time or a place — it could be anytime. It's when I'm stressed, or when something stressful has happened, or when I'm down. If that's you, you are not wrong that the feeling is there — but it is worth looking underneath it. Stress-eating is real, yet much more often the stress is happening inside a familiar set of circumstances where the conditioning has already been laid down. Because a feeling is something you are conscious of — and because there is so much cultural folklore about emotional eating — it is easy to credit the episode to the stress and file it away, while the quieter driver underneath was the same cue-triggered wanting, built up over many past pairings in that particular setting. The invitation is not to talk yourself out of the stress, but to look for the cues sitting beneath it: where were you, what time was it, what was around you?
Noticing and recognizing
The primary skill is simpler than it sounds: notice and recognize wanting when it arrives. The next time you find yourself in one of your high-risk settings, the invitation is only to pause — look around, take a beat, look at the time — and ask yourself how many times this setting has been paired with reward-value food. Recognize the response for what it is: not physical hunger, but wanting — cue-triggered attention bias, the central symptom. You are not being asked to stop it or change anything. Noticing it, and naming the setting as one of your high-risk times, is the work.
Recognizing wanting — and the high-risk times that trigger it — is the central skill in weight management.
A more involved exercise called urge surfing — deliberately riding the wave of wanting until it crests and falls on its own — also exists, and can help some people experience wanting as something that passes without being acted on. It is used sparingly. Noticing and recognizing has largely superseded it, and deliberately riding out an urge can be intimidating or difficult for some people — particularly early in medication, or at a low dose after weight loss. Where it is used at all, it follows comfortable recognition, not before it.
Understanding wanting and its significant impact on eating behaviours, calorie intake, and weight is an important first step. In the modules to come, you will learn behavioural and cognitive techniques to help you avoid wanting where possible, minimize its intensity, and manage it when it occurs. Understanding and managing wanting is significantly associated with improved weight loss outcomes.

- Berthoud HR. Blaming the Brain for Obesity: Integration of Hedonic and Homeostatic Mechanisms. Gastroenterology. 2017. View source ↩
- Petrovich GD. Lateral Hypothalamus as a Motivation-Cognition Interface in the Control of Feeding Behavior. Frontiers in Systems Neuroscience. 2018. View source ↩
- Elks CE et al. Variability in the heritability of body mass index: a systematic review and meta-regression. Frontiers in Endocrinology. 2012. View source ↩
- Locke AE et al. Genetic studies of body mass index yield new insights for obesity biology. Nature. 2015. View source ↩
- Carr KA, Lin H, Fletcher KD, Epstein LH. Food reinforcement, dietary disinhibition and weight gain. Appetite. 2018. View source ↩